Anatomy and Physiology of the Interproximal Zone
The interproximal zone — an anatomical and functional entity
The interproximal zone (IPZ) is a pyramidal anatomical entity whose base is the alveolar septum — cancellous bone bounded by the alveolar walls of adjacent teeth and the buccal and lingual cortical plates. Its apex is defined by the interdental contact point, which is punctiform in young patients and becomes a contact surface in adults due to physiological proximal wear.
The gingival papilla divides into buccal and lingual aspects separated by the interdental col — a critical zone of vulnerability devoid of keratinization, not subject to direct mechanical stimulation, and highly permeable to bacterial toxins.
Functions of the contact point
- Protecting the papilla from direct food impaction
- Guiding tooth eruption
- Transmitting occlusal forces along the dental arch
- Maintaining the integrity of the underlying alveolar septum
Physiological self-cleansing
- Marginal ridges and occlusal fossae direct the food bolus toward the occlusal table
- Combined action of the cheeks, tongue and saliva
- Evacuation of food residues through the embrasures
- Intrinsic fragility of cancellous bone when this balance is disrupted
Etiology — Classification of Failures
Primary trigger
- Disruption of the IPZ protective balance leading to food impaction (packing)
- Three distinct origins: morphological/physiological, occlusal/functional, iatrogenic/therapeutic
- Understanding the etiology directly determines the Phase 2 corrective treatment plan
Morphological and physiological factors
Malpositions (rotations, tipping) displace or eliminate the contact point, leaving the papilla exposed. Oversized embrasures due to exaggerated coronal relief cannot be filled by the papilla. With aging, gingival recession and contact point wear increase susceptibility to food packing.
Occlusal disharmonies — kinetic forces
The plunger cusp penetrates the interdental space like a wedge during mastication. Uneven marginal ridges create a step where food debris accumulates. Occlusal interferences produce a pump effect — transient micromovement of teeth that opens the contact point. Bruxism accelerates contact surface wear and creates sharp cusp edges.
Iatrogenic causes — the paradoxical role of restorations
| Type of Defect | Technical Description | Pathological Consequence |
|---|---|---|
| Defective contact point | Absence of proximal convexity or loose contact | Free passage of food toward the papilla |
| Overhanging restoration | Restorative material beyond the cervical margin (overhang) | Plaque retention + direct mechanical irritation |
| Inadequate emergence profile | Crown over-contoured or under-contoured at the cervical margin | Papilla compression or bacterial niches |
| Inadequate finishing | Absence of proximal surface polishing | Increased calculus and food debris adhesion |
| Uncompensated extraction | No replacement of extracted tooth | Adjacent tooth migration — open spaces |
Pathogenesis — Physiopathological Cascade
From mechanical injury to bone destruction
Syndrome development follows a well-defined biomechanical cascade. Food impaction exerts pressure on the junctional epithelium of the interdental col, disrupting epithelial attachment and creating a microbial entry point. Stagnant debris ferments, providing an ideal substrate for intense bacterial proliferation. The resulting papillary edema aggravates food retention, creating a self-amplifying vicious cycle that can only be broken by mechanical debridement.
The five stages of the physiopathological cascade
Sequential progression from localized gingivitis toward periodontitis and bone lysis.
Food impaction exerts direct pressure on the junctional epithelium of the interdental col.
Rupture of epithelial attachment opens a bacterial entry point.
Fermentation of stagnant debris creates an ideal growth medium for pathogenic flora.
Initial gingival inflammation with progressive papillary edema.
Papillary edema increases food retention, which sustains the edema — self-amplifying loop.
Apical migration of junctional epithelium → progression to periodontitis.
Inflammation of the periodontal ligament and interproximal cancellous bone.
Early vertical or angular bone resorption, visible on bite-wing radiograph.
Formation of a septal micro-abscess with rapid and irreversible bone destruction.
Risk of permanent tooth loss if treatment is delayed or incomplete.
Semiology and Clinical Diagnosis
Subjective symptoms — History
- Pain triggered by mastication — sensation of pressure or tension
- Relief when dislodging food debris
- Evolution toward spontaneous, diffuse, throbbing pain — may mimic pulpitis
- Radiation to adjacent regions (risk of misdiagnosis)
- Persistent localized bad taste
- Thermal hypersensitivity from root exposure secondary to recession
Objective findings — Physical exam
- Red, edematous, congested interdental papilla
- Profuse bleeding on probing or spontaneous hemorrhage
- Putrid food debris visible on inspection
- Acute pain on bidigital palpation of the papilla (pathognomonic sign)
- Pulp vitality tests: positive and normal on affected teeth
- Lateral percussion more sensitive than axial percussion
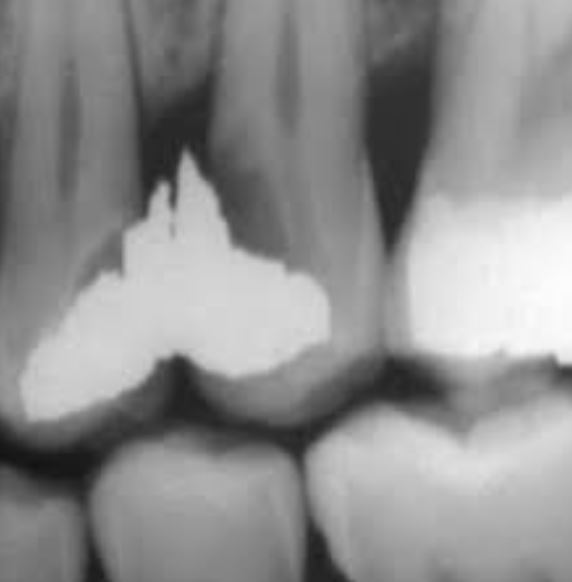
Radiographic assessment — Bite-wing as first-line investigation
- Investigation of choice: periapical radiograph using the bite-wing technique
- Loss of continuity of the lamina dura at the septal crest
- Widening of the interproximal periodontal ligament space
- Horizontal or angular bone loss, varying in depth by stage
- Identification of the etiological factor: proximal caries, overhang, contact defect
Differential Diagnosis
Navigating orofacial pain — Comparative table
| Criterion | Septum Syndrome | Irreversible Pulpitis | Acute Apical Periodontitis | Periodontal Abscess |
|---|---|---|---|---|
| Trigger | Meals / papilla palpation | Spontaneous, nocturnal | Axial percussion | Variable, diffuse |
| Pain duration | Subsides after food removal | > 30 sec after stimulus | Continuous, throbbing | Persistent |
| Pulp vitality | Positive, normal | Exaggerated | Negative | Variable |
| Tooth mobility | Absent | Absent | Slight | Marked |
| Pain location | Interdental, localized | Dental, radiating | Apex — "high tooth" | Diffuse gingival |
| Radiology | Septal bone loss | Usually normal | Periapical lesion | Pre-existing pocket |
Spontaneous pain, often nocturnal, worsened in recumbent position, lasting more than 30 seconds after thermal stimulus. An endodontic treatment performed in error on a vital tooth is definitively irreversible.
Pain linked to meals, relieved by food removal. Pulp vitality test positive and normal. Pain on bidigital palpation of the papilla. Treatment is periodontal, not endodontic.
Exquisite pain on axial percussion, sensation of "high tooth," tooth often non-vital or undergoing necrosis. Periapical lesion visible on radiograph. Lateral percussion not significant.
Pulp vitality preserved and normal. Pain centered on the interdental space. Lateral percussion more sensitive than axial, revealing preferential involvement of the interproximal ligament.
Three-Phase Treatment Protocol
Removal of food debris by irrigation or gentle curettage.
Near-immediate relief after complete food removal.
Subgingival curettage under local anesthesia — removal of calculus and necrotic tissue.
Irrigation with chlorhexidine or hydrogen peroxide (H2O2). Topical application of eugenol.
Analgesics + NSAIDs per os according to pain VAS score.
Antibiotics only if systemic signs present: fever, cervical lymphadenopathy.
Replacement of defective restorations with strict proximal anatomy reconstruction.
Elimination of any overhang — systematic finishing and polishing.
Selective grinding of plunger cusps and uneven marginal ridges.
Restoration of a physiological food bolus pathway.
Crowns, bridges or implants for mesiodistal support loss.
MM-DD technique for posterior implants — MDA crowns to restore contact without full prosthetic replacement.
Teaching systematic use of interdental brushes sized to the embrasure diameter.
Alternative: dental floss with correct C-shaped technique around each tooth.
Regular check-up visits — periodontal status and integrity of restored contact points.
Periodic bite-wing radiographs for early detection of any recurrent septal bone loss.
Medications and Prescriptions
Ibuprofen
Paracetamol
Chlorhexidine
Amoxicillin
Evolution and Systemic Complications
Locoregional complications
- Continuing bone loss → irreversible mobility → tooth loss
- Cementum and proximal caries in acidic stagnation zones
- Retrograde pulpitis if periodontal infection reaches the apical foramen
- Periodontal abscess formation on a pre-existing pocket
Systemic risks
- Infective endocarditis in at-risk cardiac patients
- Glycemic imbalance (HbA1c) — bidirectional relationship with diabetes
- Maxillary sinusitis by extension (posterior maxillary sector)
- Distant abscesses (pulmonary, cerebral) in severe neglected cases
Chronic inflammation of the interproximal zone can destabilize glycemic control, measured by HbA1c. A neglected septum syndrome in a well-controlled diabetic patient may render glycemic management impossible despite optimal pharmacological treatment.
Systematically screen for septum syndrome signs in every diabetic patient. Complete periodontal debridement directly contributes to improved glycemic control — a shared therapeutic goal with the treating physician.
Special Patient Populations
Children and primary dentition
- Syndrome commonly occurs between primary molars after untreated proximal caries
- Intense pain that may impair feeding and affect growth
- Early caries treatment restores the contact point and provides immediate relief
- Not to be underestimated: a genuine functional emergency
Implant patients
- The implant, lacking a periodontal ligament, does not follow the physiological mesial drift
- Creates open spaces ("black triangles") and insufficient contact points
- MM-DD technique: proactive occlusal adjustment to close open spaces
- MDA crowns: restoring contact without full prosthetic replacement